There's a particular kind of silence that falls in a consultation room just before a difficult conversation begins.
It's the silence that comes when the scan results are not what we hoped. Or when a patient says, "Just tell me what the scan shows," and you know that what you're about to say will land like a stone. It's not something we're trained for with mnemonics or simulated OSCEs. And yet, it's precisely in those moments, when a patient is struggling to find words, or when we realise ours might wound rather than heal—that the art of medicine is most needed.
We talk a lot about evidence-based practice. But what about meaning-based practice?
In the traditional model of medical education, these moments are often left to be picked up "on the job," or absorbed through osmosis. We front-load the science: anatomy, physiology, pharmacology. And when we do include the humanities, if at all, they're slotted in as an elective, or a feel-good session on Friday afternoons. Something nice. Optional. Decorative.
But what if we've been treating the humanities like dessert when they are, in fact, part of the main course?
The Case for Integration
A not so recent monograph from the AAMC titled The Fundamental Role of the Arts and Humanities in Medical Education makes a compelling case: we need the humanities not as a feel-good, Friday-afternoon elective, but as a foundational part of how we train and sustain doctors. They argue that to meet the 21st-century demands of medicine—burnout, inequity, misinformation, pandemics—we need doctors who are not only scientifically literate but emotionally agile, reflective, and ethically grounded.
The world of medicine today is complex, fast-changing, and often overwhelming. It is a world of technological wizardry and deep uncertainty. Of remarkable cures and deep suffering. Of moral fatigue, burnout, inequality. The AAMC suggests that to truly equip doctors for these realities, we must teach them to see not just with the eyes, but with imagination. To listen not just for the symptom, but for the story. To act not just with precision, but with wisdom.
The Four Functions That Transform Practice
The arts and humanities, the report suggests, aren't fluff. They're functional. The AAMC's commissioned research led to what they call the Prism Model—a framework that identifies four key functions of arts and humanities in medical education, each offering a different yet interrelated way of seeing arts and humanities teaching, most powerful when used in combination.
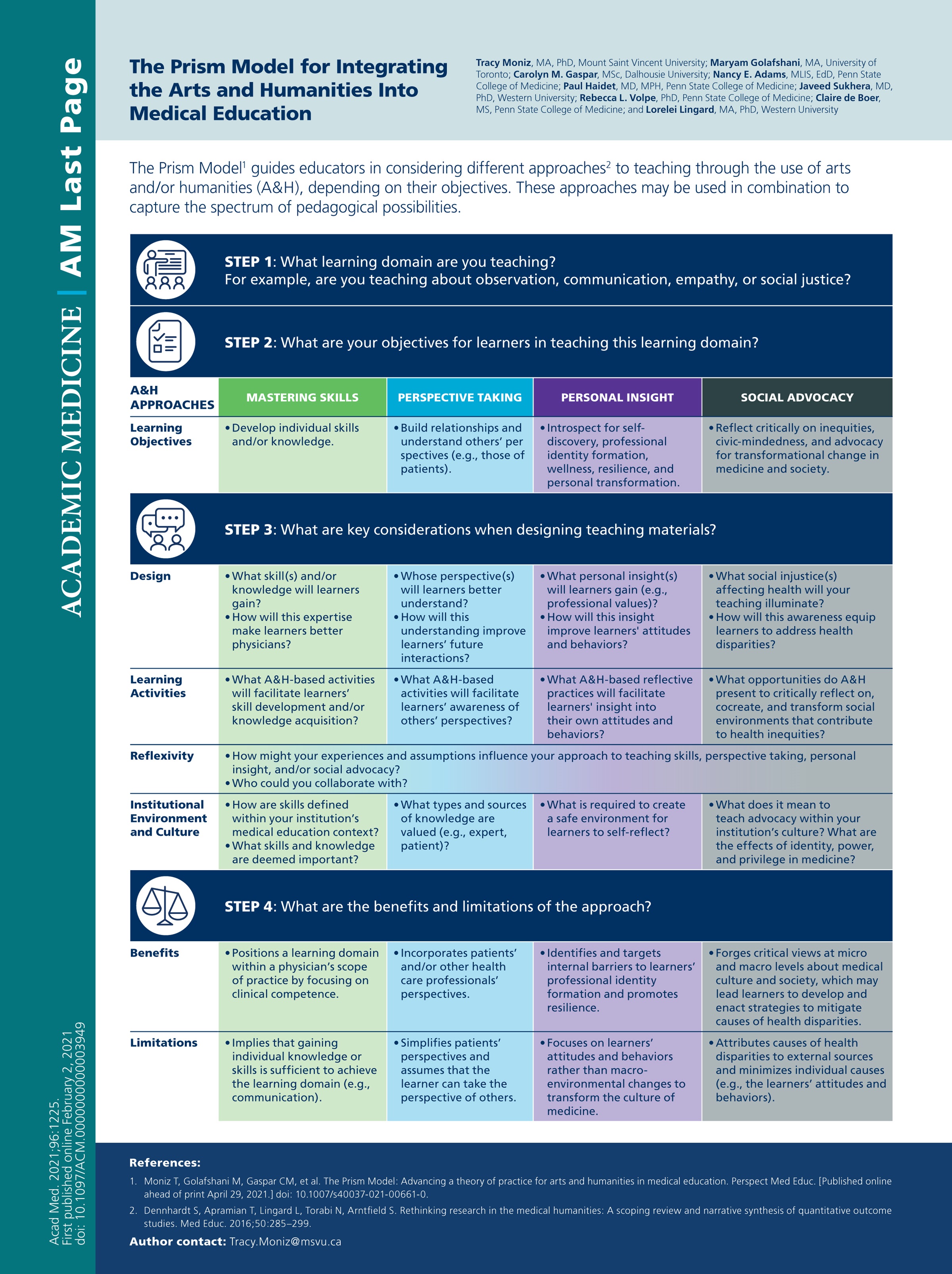
They help us:
Master clinical skills (yes, even physical exam skills through art observation). Take Harvard Medical School's "Training the Eye" course, where students learn visual observation skills through art analysis before applying them to physical diagnosis. Students become more attuned to posture, gait, facial expression which are the subtle clues that tell us something is not quite right. It's not just about looking; it's about learning to see.
Foster perspective-taking (essential for working in teams, with patients, across cultures). At East Carolina University, their Medical Readers' Theater has students perform adapted short stories about medical ethics for public audiences, followed by community discussions. It's one thing to read about bias or injustice in a textbook. It's another to feel it reverberate through a character's voice and then listen as real patients, community members, and colleagues respond.
Gain personal insight (hello, professional identity formation and burnout prevention). Programs like the Veterans Affairs' "My Life, My Story" initiative have medical trainees interview patients about their life narratives, then place these stories prominently in medical records. Suddenly, a patient with multiple comorbidities becomes a father, a teacher, a poet. Documentation becomes humanization.
Drive social advocacy (because sometimes you have to name the wound before you can treat it). At Johns Hopkins, students explore the history of medicine through a critical lens, examine racialized public health policies during historical epidemics and draw connections to contemporary challenges. They learn that public health is never neutral, that every data point lives in a social context, that history repeats unless we are brave enough to name it.
Beyond Columbia's Narrative Medicine
It's not just Columbia's Narrative Medicine program (though they deserve the shoutout). It's jazz and the art of improvisation in clinical communication at Penn State, where students learn that real-time translation of basic communication elements mirrors what jazz musicians do when they play together. It's drawing from comics, literature, and dance to explore grief, joy, disconnection, and healing. It's veterans' life stories, entered into the EMR, because sometimes what matters most about a patient isn't their creatinine.
At Northwestern's "Playing Doctor" course, medical students engage in improvisational theater techniques to develop cognitive flexibility, emotional honesty, and clear communication. The primary goal is developing concrete skills that embrace discovery, spontaneity, humility, confidence, and collaboration—skills essential for navigating the unpredictable nature of clinical practice.
And yes, it's also about asking questions that don't have single right answers.
What We've Learned on the Ground
We've seen this transformation firsthand here in Singapore. Our own initiatives in narrative medicine—whether through reflective writing, facilitated storytelling, or arts-based workshops have shown time and again that clinicians are hungry for something more than checklists and dashboards. They want to listen better. Understand better. Be better.
Through our poetry workshops and reflective groups, we've witnessed healthcare workers who are desperate to make meaning from their experiences. Not just to perform well, but to feel well. To be seen. To reconnect with why they chose this path in the first place.
In an age where doctors are asked to do more with less time, less certainty, less emotional bandwidth—the humanities remind us that medicine is not just a science of the body. It is also a practice of attention, of listening, of seeing, of being with.
The Real Curriculum
This is the real curriculum. The hidden one. The one that teaches us how to be with others, and with ourselves, when knowledge runs out. The one that helps us hold our own fallibility, not with shame, but with grace.
But to do this well, we need more than goodwill. We need institutional support, rigorous evaluation, and serious scholarship. The research is clear: we must stop treating humanities teaching as an extracurricular hobby and start resourcing it as the evidence-informed pedagogical work that it is.
So maybe it's time we stopped asking whether we can "fit" the humanities into our already-packed medical curricula. Maybe we should be asking: how can we afford not to?
The vast majority of U.S. medical schools—94% as of 2018—already incorporate arts and humanities to varying degrees. The question is no longer whether the humanities belong in medical education. The question is: how did we ever think we could do without them?
As Hippocrates once said, "Wherever the art of medicine is loved, there is also a love of humanity." That feels like a good place to start.
And that kind of knowing comes not from memorizing more—but from remembering what it means to be human.
🩺 If you’re looking for more bite-sized doses of medical humanities, check out #MH101 every Monday on SDMHI’s Instagram. It’s a weekly series where our Med-Ed Team unpack tiny, powerful moments from medicine—one story, quote, or reflection at a time.
Dr. Victoria Ekstrom is a consultant gastroenterologist at Singapore General Hospital and co-lead for Narratives in Medicine at the SingHealth Duke-NUS Medical Humanities Institute. Her work explores the intersections of clinical practice, communication, and the human stories that shape healthcare.